Clinical service lines: multiple specialists, one clinic visit

When a patient copes with congestive heart failure and requires care from different specialists, he doesn’t need the added strain of traveling from doctor to doctor, getting treatment piecemeal at different appointments and worrying about communication between his providers.
A clinical service line approach at the University of Mississippi Medical Center, however, brings together as a team the caregivers a patient needs to achieve efficient, cohesive treatment for the many conditions that can accompany a complex disease. The Medical Center, unlike any other provider in the state, houses all specialties and sub-specialties in the same campus system, making it possible for a patient to see multiple physicians and other team members in one coordinated visit.
It’s much like a relay team in which one provider passes the baton to the next, with a goal of giving the patient the best experience, and communication between providers that is regular and seamless. The approach: Create a multidisciplinary clinic within a clinic.
“It’s lines of service that are coordinated and patient-centric,” said Dr. Richard Summers, associate vice chancellor for research and professor of emergency medicine. “It’s not unusual for a patient’s diagnosis and treatment to involve several providers from multiple departments. This can entail multiple visits to UMMC for initial visits, medical tests, procedures and follow-up care.”
One example: A patient’s treatment might involve a surgeon, a radiation oncologist, a medical oncologist, a nutritionist, a pharmacist and others at UMMC’s Cancer Institute. Why not see more than one of them at the same appointment?
That approach sets the stage for multiple providers and their current staffs to come together in carrying out what could be months or years of treatment. The Medical Center is embarking on clinical service lines in four initial fields: oncology, cardiovascular, transplant and orthopaedics.

“It’s almost like Disney World,” said Dr. Scott Stringer, professor and chair of the Department of Otolaryngology and Communicative Sciences and chief physician executive for UMMC’s Council of Clinical Chairs. “The patient might not know what’s going on behind the scenes, but you are presenting to them an experience.”
Service lines don’t work for all patient care, he said. “It’s best for the patient when the care requires an interdisciplinary approach involving multiple specialties and multiple specialists,” said Stringer, who also sits on the Clinical Service Line Advisory Board. “The idea is rather than have the patient navigate the whole thing, bring the service to the patient instead, in a very seamless way.”
Clinical service lines “combine a compilation of different disease types that fall within certain disease categories,” said Liz Youngblood, CEO of the Adult Hospitals and metro-area UMMC clinics. “For example, the cardiovascular service line includes diagnoses related to the heart and vascular system. Clinical service lines pull together providers from different specialties around similar disease processes.”

The focus isn’t just on outcome of treatment. “We’re going to grow our services and change the way we’re providing care,” Youngblood said.
At an academic medical center, Summers said, care is typically organized by departments. That separates specialists, requiring patients to make separate appointments. “A service line allows the patient to get multiple services naturally,” he said. “You don’t want to see one doctor and go back home, then come back and see another doctor and go back home.”
The Cancer Institute is putting the finishing touches on its reorganization as a clinical service line, said Dr. John Ruckdeschel, the institute’s director and Ergon Chair in Cancer Research. “We want to get it under one management scheme so that we can organize it in a way that makes sense for the patient.”
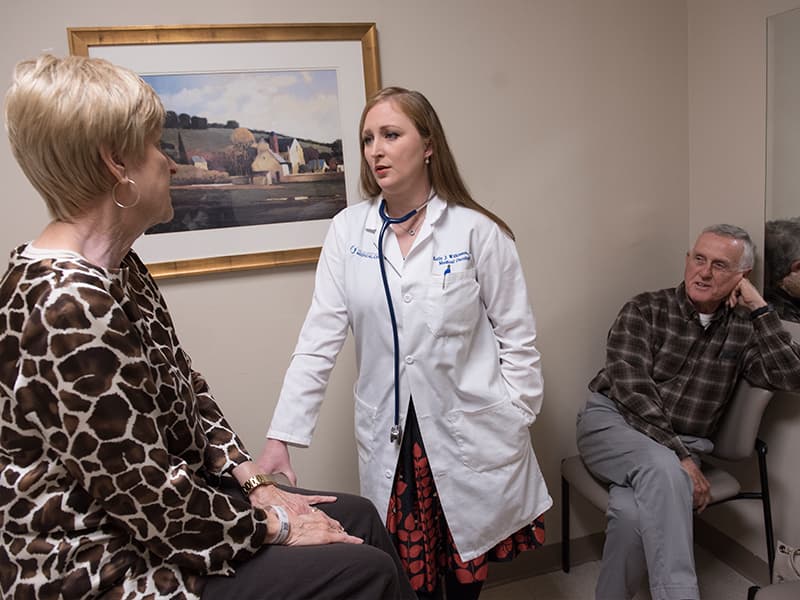
Brandon resident Ann Anderson has been giving ovarian cancer the cold shoulder for more than a decade. On Wednesday, she saw three of her caregivers – her oncologist, Dr. Kelly Wilkinson, assistant professor of hematology, plus a pharmacist and social worker – during one Cancer Institute visit.
“It was good,” said Anderson, 77, who with husband Kenneth has a daughter and three grandchildren. “I’ve been going to Grants Ferry for my blood work,” but Wednesday that was done at the Cancer Institute, saving her a trip.
She was hospitalized at UMMC for a round of chemotherapy and now is being treated with oral chemo. “I get a scan every two to three months,” said Anderson, who retired from UMMC as a physical therapy educator and also worked as a home health administrator and in clinical physical therapy.
One example of a strategy used in a clinical service line is care for UMMC patients coping with craniofacial defects.
“Because they have multiple needs, a team of specialists comes together once a month to see this group so that they can address all of their needs,” said Dr. Ron Caloss, associate professor of oral and maxillofacial surgery and pathology in the School of Dentistry. Those providers could include an ENT specialist, plastic surgeon, oral-maxillofacial surgeon, dentist or orthodontist, and speech pathologist.
The care strategy could involve combining multiple surgeries into one so that the patient has to go under anesthesia just once. “Sometimes, the care is so complex that more than one person needs to be involved in the surgery,” Caloss said.
Enhanced communication is a huge benefit that comes with more frequent, face-to-face discussions that happen within a clinical service line. For example, everyone on the team has access to the patient’s lab work, X-rays and physician’s notes in their electronic chart. “This brings a level of organization and order,” Summers said.
The new model of care will require a learning curve, Summers said. And although it’s not a main goal, there’s a cost savings because of the efficiency of doctors seeing patients during one visit and improved billing. “Hopefully, that’s also a quality driver,” Summers said.
“We’re having a lot of ‘lo and behold’ moments – ‘Wait a minute. That’s easy to fix,’” Ruckdeschel said. “It makes it so much easier for the patient, and so much easier for the staff.”