



UMMC provides patient-centered treatment, clinical excellence, and an advanced level of care unavailable anywhere else in the state.

for Kids.
Children’s of Mississippi is here for every child
with the state’s only children’s hospital
plus clinics statewide.
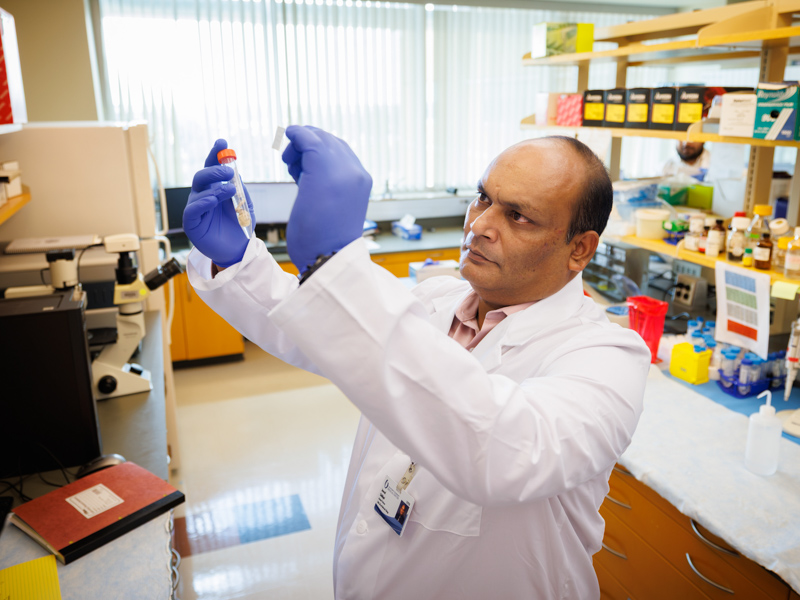
UMMC Cancer Center and Research Institute gains nearly $2.6M from NCI for metastasis research
Monday, August 10, 2026
Led by Dr. Jawed Siddiqui, this research reflects CCRI’s growing strength in translational science and the pursuit of discoveries that can change outcomes for patients across Mississippi and beyond. Read More

Photos: UMMC welcomes students for a new academic year
Monday, August 10, 2026
A new academic year is underway at the University of Mississippi Medical Center as students across UMMC’s health professions schools return to campus and begin the next chapter of their educational journeys. Read More
Latest Articles

UMMC’s inaugural MD-MPH students aim to transform health beyond the exam room
Published on Monday, August 10, 2026

Front and Center: Geneva Lindsey
Published on Monday, August 10, 2026

A first for Mississippi, a second chance for UMMC patient with rare type of cancer
Published on Monday, August 3, 2026

UMMC student connects beauty pageants to medicine
Published on Monday, August 3, 2026

UMMC Greenwood preserves access to health care in the Delta region
Published on Monday, August 3, 2026

High risk for breast cancer calls for increased screening at CCRI clinic
Published on Monday, July 27, 2026

Front and Center: Wesley Smith
Published on Monday, July 27, 2026

School of Medicine honors alumni leaders during 2026 reunion weekend
Published on Monday, July 27, 2026


Sign Up for Consult

Connect with UMMC via new e-magazine
In CONSULT, readers will have the opportunity to learn more about the cutting-edge clinical advances, innovative educational programs and groundbreaking research occurring at UMMC. Plus, CONSULT will regularly showcase our experts' best advice for living a healthy and mindful life.