Five Questions
Good morning!
It seems like 2018 is in full swing and New Year’s is just a fading memory. I’ve had a busy week with several visits to the State Capitol for meetings with legislators and other state officials.
With that in mind, I wanted to give a quick reminder that during this three-month legislative session, if you have business at the Capitol, please give a quick phone call to the Office of the Vice Chancellor so we can be aware of your activities. I love that faculty and staff of our multifaceted Medical Center are engaged in the public policy process, but I want to do that in a coordinated way so we don’t find ourselves at cross purposes. Thank you.
It’s the last Friday of the month, so today I’ll respond to your questions. As a reminder, I read all of your questions and appreciate the comments you send me. If you don’t see your question answered here, there’s a good chance I have forwarded it to our senior staff for further review.
Now, on to your questions.
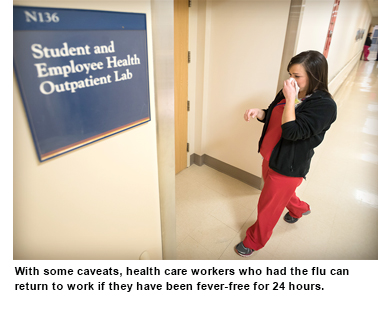 Q: How can we encourage employees to stay home when they have been diagnosed with the flu? An employee stated they no longer had a fever so they returned to work. According to the CDC, you can be contagious up to a week after diagnosis. If an employee tells their supervisor that they have been diagnosed with the flu, how can other employees be protected? It's unfair to other employees to be exposed to the flu knowingly. Can HR, Legal or Compliance research this?
Q: How can we encourage employees to stay home when they have been diagnosed with the flu? An employee stated they no longer had a fever so they returned to work. According to the CDC, you can be contagious up to a week after diagnosis. If an employee tells their supervisor that they have been diagnosed with the flu, how can other employees be protected? It's unfair to other employees to be exposed to the flu knowingly. Can HR, Legal or Compliance research this?
A: That’s a very timely question! I asked Dr. Joyce Olutade, medical director of Student and Employee Health, for guidance. Her response: A health care worker who had a recent flu infection and has not had a fever for at least 24 hours without the use of acetaminophen or other fever-reducing medications may return to work. However, those with ongoing respiratory symptoms should be evaluated by their primary care physicians or Student and Employee Health for clearance before they return to work, even if their fever has subsided. If the employee is working in a unit with immunocompromised patients (chemo unit, bone marrow transplant unit, NICU, etc.), he or she should be excluded from working directly with patients and given temporary assignments. The exclusion period is seven days from onset of symptoms or until resolution of symptoms, whichever is longer. The detailed CDC guidance to prevent the spread of flu infection in health care facilities can be found here.
Q: UMMC makes a sincere effort to encourage employee career development. Yet the retirement policies punish employees if they transition from staff to faculty. At least two individuals in my department who both prefer the Optional Retirement Plan (ORP) have faced the dilemma of remaining in PERS (Public Employees’ Retirement System) or losing the university's contribution forever (and their own contribution until they separate from UMMC) if they join the ORP. Why can't employees roll over prior PERS contributions to their ORP account? Or as an alternative, can policies be amended to allow non-faculty researchers to join ORP at their hiring?
A: As best we can determine, the laws that govern the Optional Retirement Plan for the Mississippi Institutions of Higher Learning are set in statute by the Mississippi Legislature and further explained in the ORP Plan Document, which is developed by PERS and can be found here. All Mississippi public universities are required to follow the laws established for ORP, and matters such as eligibility, contributions and distributions are beyond the purview or control of UMMC. Further, according to state law, as you indicate, no member of PERS may receive a refund of the employer’s contributions, and PERS members may not refund or roll over employee contributions to any other retirement plan unless they have terminated from PERS-covered employment. If you have additional questions, you might want to contact our benefits office.
Q: In a response in a recent VC Notes, you commented that in 2017, "We made targeted compensation adjustments to staff who are the furthest from their respective market averages.” While that is fantastic news to all of those frontline clinical staff, those of us in a salaried position who serve a vital educational role, or the program assistants who serve those efforts, have not seen any compensation adjustments in years. This is disheartening, to say the least. I fully realize the financial constraints that 2017 brought. However, moving forward as you continue to make "regular compensation reviews," I encourage you to also look to the market to see how your staff in educational roles are compensated.
A: I have received several questions via VC Notes about staff compensation during the last few weeks, so I know this is on many people’s minds. The compensation changes we are implementing this month are in response to the market and affect about two-fifths of our workforce, mostly in clinical roles. The annual cost of that increase to UMMC is about $14 million. Most other nonclinical staff have not received a general market adjustment since November 2014. I am hopeful that we will have a better financial year in FY2018, in terms of favorable revenue from all sources and continued management of expenses, so that we can take similar action for other segments of our workforce. Appropriately compensating our valued workforce is a priority. And as I have said in earlier columns and as you reference above, I am committed to regular compensation reviews that will include staff from all mission areas, including education and research.
Q: I recently experienced a medical emergency in my office with one of my coworkers who had a seizure at her desk. Fortunately, there was a resident nearby who helped me. When we dialed "0" to get a Rapid Response Team called to the office, we were transferred to several different people, including Physical Facilities. Eventually, the resident called the ED and a nurse with a wheelchair arrived to transport my coworker to the ER. After the event, I looked on the Intranet to find out who to call for medical emergencies. I could not find any phone number. What if a coworker is found slumped over on their desk? Or sustains a fall or a burn and needs immediate medical attention? What is the proper protocol to summon an emergent medical team?
A: I’m sorry about our colleague, but glad he or she got appropriate attention. This may be stating the obvious, but it bears repeating: In a hospital area, staff need to call a Code Blue/13 in such situations. For all other areas, call 911 on a campus landline or use one of the emergency call stations (the ones with the blue lights) throughout campus. Campus Police monitor these lines and will help coordinate an ambulance response. Calls to 911 from a cell phone will be routed to Jackson Police Department dispatch, which is not the preferred communication channel for on-campus emergencies. Also keep in mind that for certain cardiac emergencies, portable defibrillators are strategically located throughout campus. We will see about getting this information posted to the UMMC Intranet.
Q: When I’m walking in from the stadium parking lot in the morning, I see lots of cars with stuff inside them, sometimes items that look valuable. (I promise, I’m not casing them!) This seems like an open invitation to a burglar. Sometimes I want to leave a note that says “What are you thinking?” I hope you will share this so people will be more careful.
A: Our Campus Police report they have seen an increase in employees and students failing to lock their vehicles or leaving doors and trunks completely open. They have also noted some cars are being left with keys in the ignition. Most vehicle owners tell officers they were rushing to work or class and just didn’t think about securing their cars or their property. Our police have seen wallets, purses and other valuables in plain view, which is enticing for a criminal – even if he or she is just transiting our parking area to another part of town to burglarize. Please take the time to secure your vehicles AND your valuables, and let’s keep our parking areas safe.
Again, thanks for all of your comments and questions. Your concerns and suggestions are important to me, as we continue together on this journey toward A Healthier Mississippi.